What Causes Bipolar Disorder? Genetics, Calcium Channels, Inflammation and Brain Biochemistry
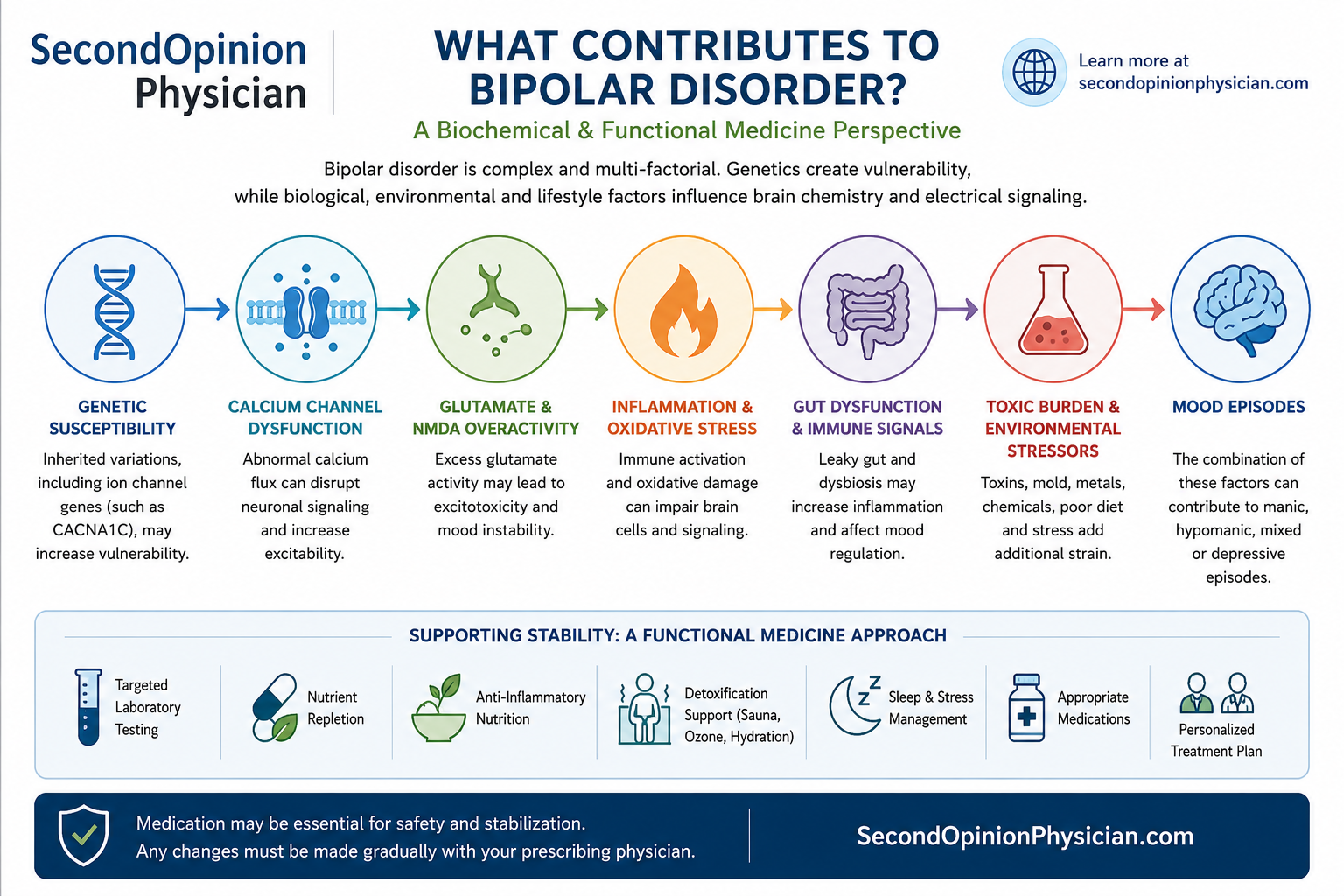
Bipolar disorder is unlikely to result from one defective neurotransmitter or one abnormal gene. A more complete model involves inherited susceptibility, unstable ion-channel signaling, stress, inflammation, oxidative injury, glutamate activity, mitochondrial function, nutrition and environmental burden.
Is Bipolar Disorder Simply a Chemical Imbalance?
Bipolar disorder is usually described as a condition involving recurring episodes of depression, mania, hypomania or mixed symptoms. That description is useful for diagnosis, but it does not fully explain why the disorder develops or why symptoms may remain absent for years before appearing.
It also does not explain why one person responds well to lithium, another responds better to lamotrigine, and another develops severe side effects without adequate mood stabilization.
Modern research increasingly points toward an interacting network of genetic, electrical, inflammatory, metabolic and environmental factors. Dr. William J. Walsh has proposed a particularly interesting version of this model in his book The Essence of Bipolar Disorder: Based on Progress in Neuroscience and Genetics.
What Does Dr. William Walsh Propose About Bipolar Disorder?
Dr. Walsh presents bipolar disorder primarily as an ion-channel disorder, or channelopathy. His theory proposes that inherited weaknesses affecting ion channels may impair the regulation of electrical signaling and neurotransmission.
He further proposes that progressive DNA damage and epigenetic changes may add to this inherited vulnerability over time, helping explain why bipolar disorder often becomes apparent later rather than being fully expressed at birth.
Ion channels are proteins that regulate the movement of charged particles—including calcium, sodium and potassium—across cell membranes. Neurons depend on these precisely controlled movements to fire, release neurotransmitters and return to a stable resting state.
Walsh's theory offers a possible framework for understanding the alternating nature of bipolar disorder: the same unstable regulatory system may shift toward excessive activation during mania and inadequate or disorganized signaling during depression.
Is Bipolar Disorder Genetic?
Bipolar disorder has a strong hereditary component, but there is no single “bipolar gene.” The condition is polygenic, meaning that many genetic variations may each contribute a small amount of risk.
Some of the most consistently studied genes influence voltage-gated calcium channels. One example is CACNA1C, which provides instructions for a major component of the CaV1.2 L-type calcium channel. Variants involving CACNA1C have been associated with bipolar disorder and several other psychiatric conditions, but they increase susceptibility rather than determining a person's destiny.
Inherited susceptibility
Genetic variations may make neuronal signaling, stress response, immune activity or cellular repair less resilient.
Epigenetic regulation
Stress, nutrition, inflammation, sleep disruption and environmental exposures can influence which genes are more or less active.
Accumulated cellular stress
Oxidative injury and impaired repair may gradually expose a vulnerability that was previously compensated for.
This helps explain why family members can carry similar susceptibility while showing very different symptoms—or no bipolar illness at all.
How Could Calcium-Channel Dysfunction Affect Bipolar Disorder?
Calcium is more than a bone mineral. Inside neurons, calcium is a powerful signaling molecule. When a neuron is activated, calcium enters through regulated channels and helps initiate neurotransmitter release, gene expression, energy production and other cellular responses.
Too little signaling may impair normal communication. Excessive, prolonged or poorly timed calcium entry can contribute to neuronal hyperexcitability, oxidative stress, mitochondrial strain and abnormal neurotransmitter release.
This calcium-flux model does not mean that serum calcium is necessarily high. Blood calcium and calcium movement through neuronal ion channels are different issues. A normal metabolic panel does not rule out abnormal intracellular calcium signaling.
Magnesium, vitamin D status, oxidative stress, mitochondrial health, membrane integrity and glutamate activity may all influence how calcium signals are handled. Their exact clinical importance varies from patient to patient.
What Is the Relationship Between Glutamate, NMDA Receptors and Mania?
Glutamate is the brain's major excitatory neurotransmitter. It is essential for attention, learning, memory and normal neuronal communication. Problems arise when glutamate signaling becomes excessive or inadequately balanced by inhibitory systems such as GABA.
NMDA receptors are one type of glutamate receptor. When activated, they permit calcium to enter the neuron. Excessive or prolonged NMDA-receptor activity may therefore connect glutamate overactivation directly to abnormal calcium flux, oxidative stress and cellular injury.
Possible signs of excessive excitation
- Reduced need for sleep
- Racing thoughts
- Agitation or irritability
- Sensory overstimulation
- Rapid speech or increased goal-directed activity
- Difficulty slowing the mind
Factors that may worsen excitation
- Severe sleep deprivation
- Psychological stress
- Stimulants or activating medications
- Alcohol or recreational drugs
- Inflammation and oxidative stress
- Metabolic or mitochondrial dysfunction
Does dietary glutamate increase brain glutamate?
Dietary glutamate and brain glutamate are not interchangeable. The blood-brain barrier tightly regulates glutamate entry into the brain. It would therefore be an oversimplification to claim that every glutamate-containing food directly causes mania.
Nevertheless, some patients report greater irritability, headaches, insomnia or overstimulation after highly processed foods containing concentrated flavor enhancers. A carefully observed elimination and reintroduction trial may be reasonable when the history strongly suggests sensitivity, but it should not replace stabilization or medical care.
Does Inflammation Contribute to Bipolar Disorder?
Inflammatory signaling is increasingly studied in bipolar disorder. Research has identified immune and inflammatory abnormalities in at least some patients, especially during acute episodes. However, bipolar disorder is heterogeneous, and not every patient has elevated routine inflammatory markers.
Inflammation may alter neurotransmitter metabolism, mitochondrial function, glutamate regulation, sleep, stress hormones and neuronal plasticity. It may therefore act less like a single cause and more like an amplifier of an already vulnerable nervous system.
Immune activation
Cytokines may alter mood, energy, sleep and cognition.
Oxidative stress
Reactive molecules may damage membranes, mitochondria and DNA.
Glutamate effects
Inflammation may disturb glutamate production and clearance.
Reduced resilience
Inflamed neurons may tolerate stress and sleep loss less effectively.
Potential inflammatory contributors include obesity, insulin resistance, poor diet, dental disease, autoimmune activity, gut inflammation, chronic infection, sleep apnea, smoking and selected environmental exposures.
How Do Stress and Sleep Loss Trigger Bipolar Episodes?
Genetic susceptibility does not operate in isolation. Many episodes follow prolonged stress, disrupted sleep, travel across time zones, postpartum hormonal changes, substance use, medication changes or major emotional events.
Sleep loss is particularly important because sleep disruption can both result from mania and further intensify mania. Once this cycle begins, waiting for nutritional therapy alone to work may be dangerous.
Reduced need for sleep can be an early warning sign
A person who suddenly sleeps very little without feeling tired, becomes unusually energetic, starts multiple projects, spends impulsively, becomes grandiose or develops rapid speech may be entering hypomania or mania. Prompt psychiatric assessment may prevent a much more severe episode.
Can Gut Health Affect Bipolar Symptoms?
The gut communicates with the brain through immune signals, microbial metabolites, the vagus nerve, hormones and nutrient absorption. Gut dysfunction should not automatically be assumed to cause bipolar disorder, but it can add inflammatory and metabolic stress.
Clinically relevant areas may include:
Gut testing is most useful when there are corresponding symptoms or historical clues. It should not be ordered indiscriminately simply because a psychiatric diagnosis is present.
Related reading: gut health and mental health.
Are People With Bipolar Disorder More Vulnerable to Toxic Burden?
In clinical practice, some patients with bipolar disorder appear unusually sensitive to medications, alcohol, chemicals, mold exposure, sleep loss and metabolic stress. This does not prove that “toxins cause bipolar disorder.” It may indicate that a vulnerable nervous system has less reserve for managing additional oxidative or inflammatory stress.
Toxic burden may include ongoing exposure, impaired elimination, oxidative injury or the metabolic consequences of chronic illness. Potential contributors can include:
Environmental exposures
Mold, mycotoxins, solvents, smoke, pesticides and occupational chemicals may warrant investigation when supported by the history.
Heavy metals
Lead, mercury and other metals can affect neurological function, but testing and treatment require careful interpretation.
Internal metabolic burden
Poor glycemic control, liver or kidney dysfunction, inflammation, oxidative stress and impaired methylation may reduce resilience.
Elevated SAH and impaired methylation
S-adenosylhomocysteine, or SAH, is a product of methylation reactions. When SAH accumulates, it can inhibit methyltransferase activity even when homocysteine is not markedly elevated. This may impair normal methylation of neurotransmitters, phospholipids, proteins and DNA.
A direct methylation panel measuring SAM and SAH may provide information that cannot be obtained from an MTHFR result alone. Read more about elevated SAH, undermethylation and creatine and methylation demand.
What does responsible detoxification mean?
Detoxification should begin with reducing ongoing exposure and supporting normal physiology—not with aggressive chelation, prolonged fasting or large supplement protocols during an unstable mood episode.
Reduce exposure
Address smoking, alcohol, contaminated environments, mold, unsafe occupational exposure and unnecessary chemical burden.
Support elimination
Maintain hydration, adequate protein, fiber, bowel regularity, movement and appropriate liver and kidney monitoring.
Improve resilience
Correct deficiencies, improve metabolic health, lower inflammation and support antioxidant defenses.
Can sauna help?
Sauna may support relaxation, circulation, sweating and cardiometabolic health in appropriately selected patients. It is not an established treatment for mania or bipolar disorder.
Dehydration is particularly concerning for patients taking lithium because fluid and sodium changes may alter lithium levels. Sauna use should therefore be conservative, well hydrated and discussed with the prescribing clinician.
What about ozone therapy?
Medical ozone has been proposed to influence oxidative signaling, circulation, immune regulation and cellular antioxidant responses. Clinical evidence for ozone as a treatment for bipolar disorder remains insufficient. It should be considered, at most, an adjunctive functional intervention for selected medical issues—not a substitute for mood stabilization.
Read more about medical ozone therapy and toxic burden management.
Which Diet Is Best for Bipolar Disorder?
There is no single diet proven to work for everyone with bipolar disorder. A practical foundation is a nutrient-dense whole-food diet that reduces large blood-sugar fluctuations, alcohol, excessive refined carbohydrates and ultra-processed foods.
Protein and amino acids
Adequate protein supports neurotransmitter precursors, glutathione, detoxification pathways and stable blood sugar.
Healthy fats
Omega-3 fats and intact food sources of fat support neuronal membranes and may complement conventional treatment.
Metabolic stability
Reducing large glucose and insulin swings may improve energy, inflammation, appetite and sleep.
Ketogenic and Mediterranean-style diets
A Mediterranean-style diet emphasizes vegetables, quality protein, legumes when tolerated, fish, olive oil, nuts and minimally processed foods. It is generally easier to sustain and supports cardiometabolic health.
Ketogenic diets are being studied in metabolic psychiatry because ketones may affect mitochondrial function, glutamate-GABA balance, oxidative stress and neuronal excitability. Early bipolar studies are promising, but the evidence remains preliminary.
Ketosis can change medication and hydration requirements
A ketogenic diet may cause early changes in fluids, sodium, glucose, appetite and medication tolerance. This is especially important for patients taking lithium, blood-pressure medication or diabetes medication. A medically supervised program is preferable.
Intermittent fasting
Intermittent fasting may improve insulin sensitivity and metabolic flexibility in selected stable patients. It may also disturb sleep, increase physiological stress or encourage erratic eating in others.
It should not be started during acute mania, severe depression, malnutrition, pregnancy or an unstable medication period. Mood and sleep stability take priority over achieving a fasting window.
Which Laboratory Tests May Be Helpful in Bipolar Disorder?
No blood test diagnoses bipolar disorder. Laboratory testing can identify modifiable abnormalities, monitor medication safety and help distinguish psychiatric symptoms from thyroid, nutritional, metabolic or toxic contributors.
| Test | Why it may matter | Clinical application |
|---|---|---|
| CBC and CMP | Evaluate anemia, macrocytosis, glucose, electrolytes, liver function and kidney function. | General assessment and medication monitoring. |
| Creatinine, eGFR and urinalysis | Assess kidney function, especially during long-term lithium use. | Identify declining renal reserve early. |
| TSH, free T4 and selected thyroid markers | Thyroid dysfunction can mimic or worsen depression, fatigue, agitation and cognitive symptoms. | Particularly important with lithium therapy. |
| Serum copper and ceruloplasmin | Evaluate copper transport and calculate non-ceruloplasmin-bound copper when clinically appropriate. | May be relevant to anxiety, agitation, hormonal patterns and oxidative stress. |
| Plasma zinc | Zinc participates in antioxidant defense, immune regulation and neurotransmitter-related pathways. | Interpret with copper, symptoms and supplement history. |
| Whole-blood histamine | Used in the Walsh framework alongside symptoms to assess possible methylation patterns. | May help distinguish undermethylated and overmethylated patterns. |
| SAM, SAH and SAM-to-SAH ratio | Provide a more direct assessment of methyl-donor availability and methylation inhibition. | Useful when methylation dysfunction or elevated SAH is suspected. |
| Homocysteine | Reflects aspects of methionine metabolism but does not fully describe SAM and SAH status. | Helps guide methylation-related nutrient decisions. |
| 25-hydroxy vitamin D | Vitamin D affects immune regulation, calcium biology and neurological function. | Correct deficiency without assuming it is the sole cause. |
| Urinary pyrroles | Specialized Walsh testing associated with zinc and vitamin B6 depletion in susceptible patients. | Requires careful specimen handling and interpretation. |
| hs-CRP and selected inflammatory markers | May identify systemic inflammation, although normal results do not exclude neuroinflammation. | Guide investigation of metabolic, immune or infectious factors. |
| Fasting glucose, insulin and HbA1c | Assess insulin resistance and metabolic effects of diet or psychiatric medication. | Particularly important with atypical antipsychotics. |
| Calcium and parathyroid hormone | Lithium can affect parathyroid function and calcium regulation. | Consider when calcium rises or symptoms suggest hyperparathyroidism. |
Review available Walsh and functional laboratory testing.
Which Nutrients May Support Brain Stability?
Nutrients should be selected according to symptoms, medication use and laboratory findings. The same supplement may help one biochemical pattern and worsen another.
Magnesium
Participates in NMDA-receptor regulation, energy production and hundreds of enzymatic reactions. Kidney function must be considered.
Vitamin D
Supports immune and neurological regulation. Supplementation is most rational when a measured deficiency or insufficiency is present.
Omega-3 fatty acids
Support neuronal membranes and inflammatory balance. Formulation and EPA-to-DHA composition may matter.
N-acetylcysteine
Supplies cysteine for glutathione production and is studied for oxidative stress and glutamate regulation.
Creatine
Supports cellular energy and may reduce methylation demand, but mood activation has occasionally been reported and warrants caution.
Zinc and vitamin B6
May be appropriate for documented deficiency or pyroluria-related patterns, with copper and safety monitoring.
Methyl donors require special caution in bipolar disorder
SAMe, methionine, methylfolate and other activating nutrients may increase agitation, insomnia or mood elevation in susceptible patients. They should not be prescribed from an MTHFR result alone. Current mood state, whole-blood histamine, homocysteine, SAM, SAH, medications and prior reactions should be considered.
Related reading: what causes undermethylation, overmethylation, copper overload, pyroluria and creatine and methylation.
Which Medications Are Commonly Used for Bipolar Disorder?
Medication remains essential for many people with bipolar disorder, particularly during mania, psychosis, mixed episodes, severe depression or dangerous instability. The appropriate medication depends on the phase of illness, prior response, medical history and side-effect risk.
| Medication group | Potential role | Important long-term considerations |
|---|---|---|
| Lithium | Acute mania, relapse prevention and long-term mood stabilization. It also has evidence for reducing suicide risk. | Kidney function, thyroid function, calcium, parathyroid effects, tremor, weight changes, hydration and drug interactions. |
| Lamotrigine | Often used for bipolar depression and prevention of depressive relapse rather than rapid control of acute mania. | Must be titrated slowly because of the risk of serious rash. Dizziness, headache and sleep effects may occur. |
| Valproate or divalproex | Commonly used for acute mania, mixed features and maintenance. | Weight gain, insulin resistance, liver effects, platelet changes, hair loss, tremor and major pregnancy-related risks. |
| Carbamazepine or oxcarbazepine | May be used for mania or selected treatment-resistant patterns. | Sodium, liver function, blood counts, skin reactions and numerous medication interactions. |
| Atypical antipsychotics | Several are used for mania, psychosis, bipolar depression or maintenance. | Weight gain, diabetes, lipid abnormalities, sedation, movement disorders, elevated prolactin and cardiovascular risk vary by drug. |
| Antidepressants | Sometimes used cautiously for bipolar depression, usually with a mood stabilizer when appropriate. | May increase activation, rapid cycling or mood switching in some patients. Biochemical fit and prior reactions matter. |
Lithium and long-term kidney health
Lithium can be highly effective, and many patients remain stable on it for years. At the same time, long-term lithium exposure is associated with impaired urinary concentration in some patients and a higher risk of chronic kidney disease in a subset of long-term users.
The risk appears to be influenced by treatment duration, age, lithium levels, episodes of toxicity, hypertension, diabetes, dehydration and other kidney stressors. Declining kidney function should not be ignored, but lithium also should not be stopped abruptly without weighing the psychiatric risk.
Nutritional therapy may improve the broader biological environment, but it does not reverse advanced lithium nephropathy or make laboratory monitoring optional.
Read: choosing the correct antidepressant through a biochemical assessment .
Stabilize First
Severe mania, psychosis, suicidal depression, dangerous impulsivity or an inability to care for basic needs requires immediate stabilization. Medication, hospitalization, structured psychiatric treatment and family support may be absolutely necessary.
The goal of biochemical and functional treatment is not to persuade an unstable patient to discontinue medication. The safer sequence is:
Only after sustained stability and correction of relevant abnormalities should a gradual, prescriber-supervised medication reduction be considered. Abrupt withdrawal can provoke insomnia, rebound symptoms, mania, depression or hospitalization.
The Second Opinion Physician Functional Evaluation
A functional evaluation of bipolar disorder does not replace psychiatric diagnosis or treatment. It expands the investigation to identify modifiable biological stressors that may influence long-term stability.
Biochemical patterns
- Undermethylation or overmethylation
- Copper and zinc imbalance
- Pyroluria-associated nutrient loss
- Elevated SAH and impaired methylation
- Oxidative stress and impaired antioxidant reserve
Medical and metabolic factors
- Thyroid and hormonal abnormalities
- Vitamin D and nutrient deficiencies
- Insulin resistance and weight change
- Kidney and liver function
- Medication adverse effects and interactions
Whole-body contributors
- Gut dysfunction and inflammatory burden
- Sleep apnea and circadian disruption
- Mold, metals or other supported exposure concerns
- Diet, alcohol, stimulants and recreational drugs
- Stress, trauma and loss of daily structure
Treatment priorities
- Maintain psychiatric stability
- Correct measured abnormalities gradually
- Reduce avoidable inflammatory and toxic stressors
- Protect sleep and circadian rhythm
- Monitor medication effectiveness and long-term safety
Frequently Asked Questions About Bipolar Disorder
What does Dr. William Walsh believe causes bipolar disorder?
Dr. Walsh proposes that bipolar disorder is fundamentally related to inherited weaknesses affecting ion channels, combined with progressive DNA damage and impaired neuronal signaling. His model emphasizes calcium flux and the regulation of neurotransmission. It remains an integrative theory rather than a universally established single cause.
Is bipolar disorder a calcium-channel disorder?
Genetic research strongly implicates several ion-channel genes, including CACNA1C, in bipolar susceptibility. This supports the concept that altered calcium signaling may contribute, but bipolar disorder is polygenic and cannot presently be reduced to one channel abnormality.
Can inflammation make bipolar disorder worse?
Inflammatory and oxidative abnormalities are found in some patients, particularly during acute episodes. Inflammation may affect glutamate, mitochondria, sleep and neurotransmitter metabolism, although it is not the only cause and routine inflammatory markers may remain normal.
Can a ketogenic diet treat bipolar disorder?
Early studies suggest that ketogenic metabolic therapy may help some patients, possibly through effects on mitochondria, glutamate, GABA and neuronal excitability. The evidence is preliminary. Medication, hydration, electrolytes and mood should be medically monitored.
Can sauna be used while taking lithium?
Sauna-related sweating and dehydration may increase lithium concentrations and toxicity risk. Patients taking lithium should discuss sauna use with the prescribing clinician, avoid dehydration and stop if dizziness, weakness, vomiting, confusion or worsening tremor occurs.
Does lithium cause kidney failure?
Lithium does not cause kidney failure in every patient. Long-term use is associated with chronic kidney disease in a subset of patients, with risk influenced by duration, age, lithium level, toxicity episodes and other medical conditions. Regular kidney monitoring is essential.
Can nutrients replace bipolar medication?
Nutrients should not replace necessary medication during mania, psychosis, severe depression or dangerous instability. Targeted nutrient therapy may help correct underlying abnormalities after the patient is stable. Any medication reduction should be gradual and directed by the prescribing physician.
Which tests are useful for bipolar disorder?
Testing may include CBC, CMP, kidney function, thyroid markers, vitamin D, glucose, insulin, copper, ceruloplasmin, zinc, whole-blood histamine, homocysteine, SAM, SAH, urinary pyrroles and selected inflammatory or gut studies. Testing should be individualized.
Investigating the Biochemistry Behind Mood Instability
Laboratory testing and a detailed clinical history may identify methylation abnormalities, nutrient deficiencies, copper imbalance, elevated SAH, medication complications, gut dysfunction and other modifiable contributors.
Selected Sources and Further Reading
- Walsh Research Institute. The Essence of Bipolar Disorder .
- Bhat S, et al. CACNA1C in the pathophysiology of psychiatric disease .
- Harrison PJ, et al. CACNA1C and other L-type calcium channels in psychiatric disorders .
- Jones GH, et al. Inflammatory signaling mechanisms in bipolar disorder .
- Choi J, et al. Sleep, mood disorders and the ketogenic diet .
- Gitlin M. Key questions on the long-term renal effects of lithium .
- Gupta S, Khastgir U. Lithium and chronic kidney disease .