What Is the Best Antidepressant for Depression? Using Biochemistry to Review Medication Fit
Second Opinion Physician is a nutrient-based mental health practice and does not promote antidepressants as the only—or necessarily the best—answer to depression, anxiety, OCD or ADHD. However, many patients arrive already taking antidepressants, antipsychotics or stimulants and want to know whether the medication is helping, making symptoms worse, or still necessary after the underlying biochemistry is addressed.
This page is designed to help patients have a more informed conversation with a psychiatrist. It does not tell patients to stop medication. The first goal is to stabilize the patient: identify urgent safety risks, continue necessary medication when the patient is severely unstable, test the relevant nutrient and biochemical patterns, begin targeted correction, and then reassess whether the medication choice and dose still make sense.
For patients with severe depression, active suicide risk, psychosis, mania, dangerous impulsivity or potential harm to others, medication may be necessary for immediate protection and stabilization. Nutrient therapy should be added as a supporting medical strategy—not used as a reason to abruptly remove treatment that is helping maintain safety.
The Questions Patients Actually Ask About Psychiatric Medication
What is the best antidepressant for depression?
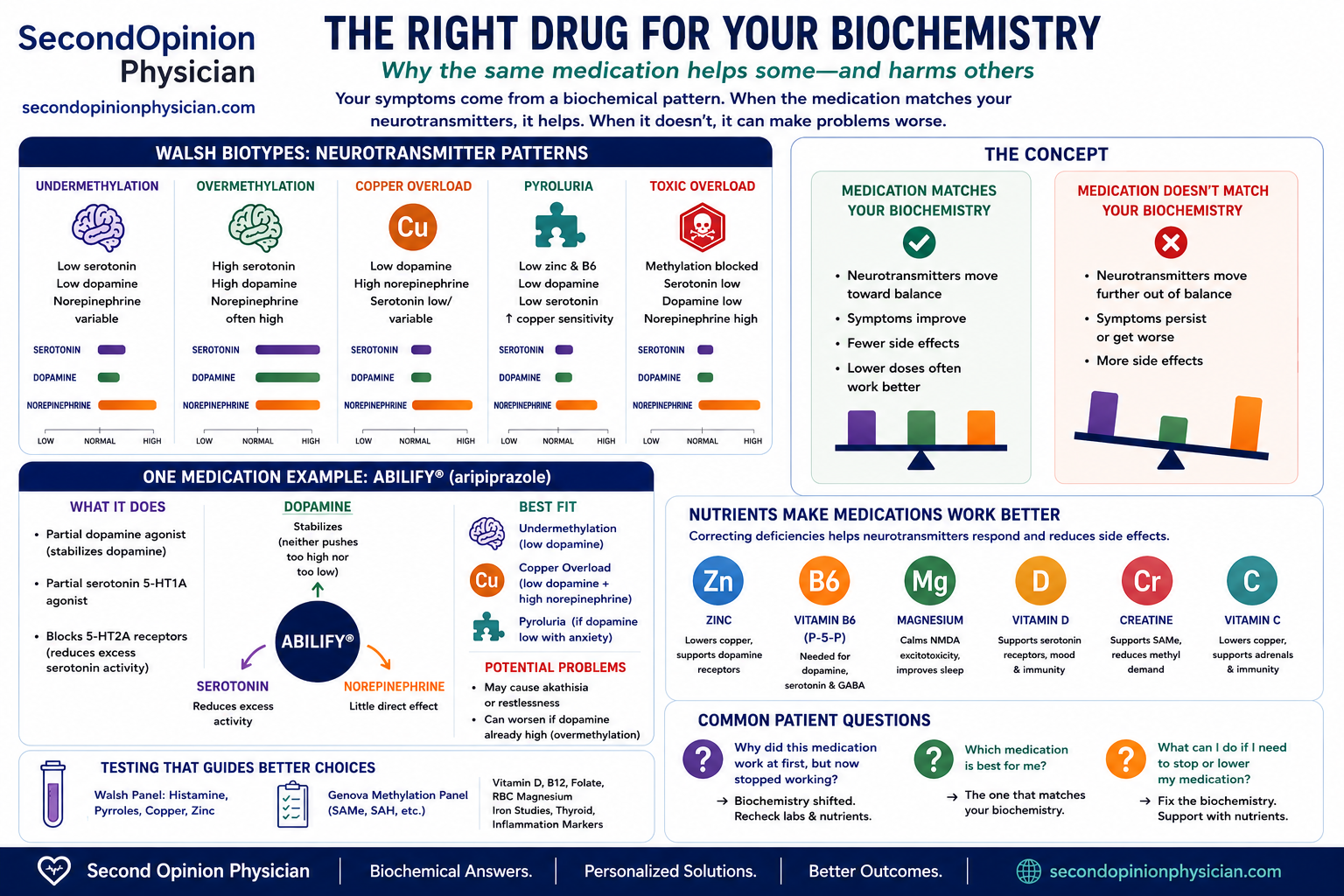
There is no single best antidepressant for every form of depression. A medication that raises serotonin may help an undermethylated, low-serotonin pattern but may aggravate an overmethylated patient who is already anxious, activated or chemically sensitive.
What antidepressant is best for an MTHFR mutation?
MTHFR status alone does not identify the best antidepressant and does not prove undermethylation. Homocysteine, MCV, whole-blood histamine, SAM, SAH, methionine and the patient’s reaction to folates provide more useful clinical context.
What is the best medication for anxiety?
Anxiety can reflect low serotonin, excessive norepinephrine from copper overload, overmethylation, pyroluria, low vitamin D, stimulant effects, withdrawal or NMDA/glutamate activation. The same anxiety diagnosis can therefore require very different medication and nutrient strategies.
What is the best medicine for ADHD?
Stimulants can improve ADHD when dopamine and norepinephrine signaling is too low in attention circuits. They may worsen panic, insomnia, irritability or palpitations when copper overload or overmethylation already produces excessive catecholamine activity.
Why did my antidepressant work and then stop working?
The medication mechanism may still be appropriate, but vitamin D deficiency, zinc/B6 depletion, copper accumulation, elevated SAH, inflammation, poor sleep, hormonal change, toxic burden or medication interactions may have altered the biochemical environment.
Could my antidepressant be making me worse?
Yes. Agitation, emotional flattening, worsening anxiety, insomnia, loss of motivation, sexual dysfunction, akathisia or cognitive slowing may indicate that the drug mechanism or dose does not fit the biochemical pattern.
Can nutrients help my medication work better?
Correcting zinc, B6, vitamin D, copper imbalance, low methionine, elevated SAH, iron deficiency, poor protein intake or toxic burden may improve the same neurotransmitter systems the medication is attempting to support.
Can nutrient treatment help me reduce medication?
Sometimes biochemical correction changes medication requirements, but medication reduction must be planned with the prescriber. The purpose of testing is to make the discussion more rational and safer—not to encourage abrupt discontinuation.
Stabilize the Biochemistry Before Considering Medication Discontinuation
The safest use of the Walsh Approach is not to remove medication first. It is to reduce the biochemical instability that made medication necessary. Many patients arrive taking several psychiatric medications because they have experienced severe depression, suicidality, psychosis, aggression, extreme anxiety, mania, dangerous impulsivity or repeated treatment failure.
Protect safety and maintain stability
When the patient is suicidal, psychotic, manic, severely agitated or potentially harmful to self or others, immediate psychiatric stabilization takes priority. A medication that is containing dangerous symptoms should not be removed simply because a nutrient imbalance is suspected.
Test the biochemical pattern
Evaluate whole-blood histamine, SAM, SAH, methionine, homocysteine, copper, ceruloplasmin, zinc, urinary pyrroles, vitamin D, CBC, CMP, thyroid, iron status and other relevant markers.
Begin targeted nutrient support
Correct documented deficiencies and imbalances gradually. This may include zinc, B6/P-5-P, vitamin D, methionine or SAMe when appropriate, creatine, antioxidant support, copper-lowering strategies, protein correction, or treatment of elevated SAH and toxic burden.
Reassess whether the medication still fits
Once the biochemical terrain is improving, review whether the current drug is still helping, whether the dose is now excessive, whether a different medication class better matches the pattern, or whether side effects were being amplified by untreated nutrient problems.
Allow time for nutrient levels to normalize
Biochemical correction is not instantaneous. Zinc, copper balance, vitamin D, methylation and pyrrole-related treatment often require repeated laboratory review and clinical observation before medication need can be judged accurately.
Taper only when stability is sustained
If symptoms remain controlled and the prescribing clinician agrees that medication need has diminished, taper slowly and monitor sleep, mood, anxiety, impulsivity, psychosis, suicidality and functional stability. Some patients can reduce medication; others continue to need it at a lower or unchanged dose.
How to Use This Page With a Psychiatrist
Bring the medication history, side effects, safety history and Walsh laboratory findings to the prescribing clinician. The prescriber can use that information to decide whether the current medication should be continued during nutrient correction, whether a better-fitting medication should be selected, or whether a later taper is reasonable after sustained stability. The diagrams use simplified directional models; they do not represent measured brain neurotransmitter levels.
Why the Same Medication Helps One Patient and Worsens Another
| Biotype or pattern | Likely neurotransmitter direction | Medication implication | Testing direction |
|---|---|---|---|
| Undermethylation | Low functional serotonin and dopamine; histamine often high | SSRIs may fit low-serotonin depression/OCD; dopamine support may fit fatigue and low motivation | Whole-blood histamine, SAM/SAH, methionine, homocysteine, zinc, B6 |
| Overmethylation | High or poorly regulated serotonin and dopamine; histamine often low | SSRIs, SNRIs and stimulants may worsen activation, panic, insomnia or emotional instability | Whole-blood histamine, methylation panel, medication sensitivity history |
| Copper overload | Low dopamine with high norepinephrine | Bupropion, SNRIs and stimulants may improve drive but worsen anxiety, panic or insomnia | Copper, ceruloplasmin, zinc and calculated free-copper pattern |
| Pyroluria | Low zinc and B6; impaired serotonin, dopamine and GABA synthesis; copper may rise | Medication may work incompletely until zinc/B6 depletion and copper imbalance are corrected | Urinary pyrroles/HPL, zinc, copper, ceruloplasmin and B6-related pattern |
| Elevated SAH / toxic burden | Methylation inhibited; neurotransmitter regulation may remain unstable | Repeated medication switches may fail while the metabolic bottleneck remains untreated | SAM, SAH, SAM/SAH ratio, homocysteine, methionine, CMP, kidney/liver clearance and toxic burden |
What Nutrient and Walsh Testing May Reveal
Low functional serotonin and dopamine activity
Medication clue: improvement with an SSRI may support the theory that low serotonin activity is important. Improvement with bupropion or a stimulant may suggest inadequate dopamine/norepinephrine signaling.
Nutrient questions: SAM/SAH, methionine, zinc, B6, vitamin D, protein intake, creatine demand and folate sensitivity.
High or poorly regulated serotonin and dopamine activity
Medication clue: activation, panic, insomnia, emotional flattening or poor tolerance of SSRIs/stimulants may fit an already overactivated pattern.
Nutrient questions: low whole-blood histamine, folate response, niacin response, medication sensitivity, copper/zinc and toxic burden.
Low dopamine with excessive norepinephrine drive
Medication clue: bupropion, amphetamine or an SNRI may improve motivation but worsen panic, insomnia, irritability or palpitations because they also raise norepinephrine.
Nutrient questions: serum copper, ceruloplasmin, plasma zinc, calculated free copper, estrogen exposure and pyroluria.
Low B6 and zinc with secondary copper imbalance
Medication clue: drugs may work only partially or stop working because B6 is needed to synthesize serotonin, dopamine and GABA, while zinc supports receptor regulation and copper balance.
Nutrient questions: urinary pyrroles/HPL, plasma zinc, B6/P-5-P status, copper/ceruloplasmin and oxidative stress.
Reduced support for serotonin biology and neuronal function
Medication clue: a medication may appear to have “stopped working” when low vitamin D, inflammation, poor sleep or another untreated contributor reduces overall brain resilience.
Nutrient questions: serum 25-OH vitamin D, magnesium, inflammation, sleep and seasonal pattern.
Methylation is inhibited despite available SAM
Medication clue: repeated medication changes may fail because the deeper problem is methylation inhibition, toxic burden, inflammation, kidney/liver dysfunction, adenosine accumulation or high creatine/glutathione demand.
Nutrient questions: SAM, SAH, methionine, homocysteine, zinc, CMP, bicarbonate/CO₂, creatine demand and toxic exposures.
If This Medication Helps—or Causes Problems—What Might It Mean?
Sertraline (Zoloft)
Primarily raises serotonin signaling by blocking serotonin reuptake.
Undermethylation with low serotonin activity, especially depression with OCD, rumination or persistent anxiety.
Overmethylation may worsen with agitation, insomnia, emotional flattening or sexual dysfunction.
Whole-blood histamine, SAM/SAH, vitamin D, zinc, B6, copper and folate response.
Escitalopram (Lexapro)
Strongly and selectively raises serotonin signaling.
Low-serotonin undermethylation with depression and generalized anxiety.
Overmethylation or low dopamine may present as apathy, low motivation, flattening or activation.
Histamine, SAM/SAH, zinc, B6, vitamin D and copper.
Fluoxetine (Prozac)
Raises serotonin and is often more activating than some other SSRIs.
Undermethylated depression with OCD traits, rumination or low drive.
Overmethylation, panic or insomnia may worsen because of serotonergic activation.
Histamine, SAM/SAH, zinc, B6, vitamin D, copper and glutamate/NMDA clues.
Bupropion (Wellbutrin)
Raises dopamine and norepinephrine with little direct serotonin effect.
Low dopamine depression: fatigue, anhedonia, low motivation, poor focus or SSRI sexual side effects.
Copper overload may already produce high norepinephrine. Bupropion can then worsen panic, irritability, tremor, palpitations or insomnia.
Copper, ceruloplasmin, zinc, pyrroles, B6, vitamin D, sleep and blood pressure.
Venlafaxine (Effexor)
Raises serotonin and norepinephrine; dopamine effect is small.
Undermethylation with low serotonin plus low energy when norepinephrine support is also useful.
Copper overload, panic, hypertension or overmethylation may worsen because both serotonin and norepinephrine are increased.
Histamine, SAM/SAH, copper, zinc, vitamin D, blood pressure and withdrawal history.
Mirtazapine (Remeron)
Raises norepinephrine and selected serotonin transmission while blocking H1, 5-HT2 and 5-HT3 receptors.
Depression with insomnia, poor appetite, nausea or SSRI intolerance.
Copper-related high norepinephrine, obesity, insulin resistance or daytime sedation.
Copper/zinc, glucose, A1c, lipids, vitamin D, sleep and appetite.
Adderall (mixed amphetamine salts)
Raises dopamine and norepinephrine by increasing release and reducing reuptake.
ADHD with inadequate dopamine/norepinephrine signaling, poor executive function, low drive or slowed activation.
Copper overload or overmethylation may cause panic, irritability, insomnia, appetite loss, hypertension or emotional overactivation.
Copper, ceruloplasmin, zinc, pyrroles/B6, vitamin D, iron/ferritin, sleep, blood pressure and heart rate.
Lisdexamfetamine (Vyvanse)
Converted in blood to dextroamphetamine; raises dopamine and norepinephrine more gradually than immediate-release amphetamine.
ADHD, executive dysfunction or binge-eating symptoms when a longer, smoother catecholamine effect is useful.
Copper overload, high norepinephrine, panic, insomnia or cardiovascular sensitivity.
Copper/zinc, pyrroles/B6, vitamin D, iron, sleep, appetite, blood pressure and heart rate.
Methylphenidate (Ritalin / Concerta)
Raises dopamine and norepinephrine mainly by blocking their reuptake.
ADHD with low dopamine/norepinephrine signaling, especially when amphetamine is too activating.
Copper overload, anxiety, tics, insomnia, poor appetite or overmethylation.
Copper, zinc, pyrroles/B6, iron/ferritin, vitamin D, sleep and thyroid function.
Aripiprazole (Abilify)
Partially stimulates dopamine D2 and serotonin 5-HT1A receptors while blocking 5-HT2A receptors.
Unstable dopamine signaling, irritability, augmentation-resistant depression or thought dysregulation where full D2 blockade may be excessive.
Akathisia, copper-related catecholamine excess or overmethylation may present as severe restlessness, insomnia or compulsive behavior.
Copper/zinc, pyrroles/B6, vitamin D, sleep and akathisia history.
Quetiapine (Seroquel)
Blocks dopamine D2 and serotonin 5-HT2A receptors and strongly promotes sedation through histamine blockade.
Excessive dopamine/serotonin activation, psychosis, mania or severe insomnia.
Undermethylation with low dopamine may worsen with apathy, cognitive slowing, fatigue and reduced motivation.
Glucose, A1c, lipids, weight, vitamin D, copper/zinc and baseline cognition.
Olanzapine or Risperidone
Strongly block dopamine D2 and serotonin 5-HT2A receptors.
Psychosis, mania, aggression or severe high-dopamine behavioral dysregulation.
Low dopamine depression or undermethylation may worsen with apathy, anhedonia, movement symptoms, sexual dysfunction or emotional flattening.
Glucose, A1c, lipids, weight, prolactin, vitamin D, copper/zinc and movement symptoms.
If a Medication Works, Which Nutrients and Labs May Support the Same System?
| Medication response | Possible biochemical clue | Labs and nutrients to investigate |
|---|---|---|
| SSRI improves depression, OCD or rumination | Low functional serotonin activity or undermethylation may be important. | Whole-blood histamine, SAM/SAH, methionine, zinc, B6, vitamin D, protein intake and folate sensitivity. |
| Bupropion improves motivation and energy | Low dopamine/norepinephrine activity may be important. | Copper/ceruloplasmin, zinc, B6, vitamin D, iron/ferritin, thyroid and sleep. |
| Stimulant improves ADHD and executive function | Prefrontal dopamine/norepinephrine signaling may be inadequate. | Copper, zinc, B6, iron/ferritin, vitamin D, sleep quality, protein intake and thyroid function. |
| Antipsychotic reduces psychosis, mania or aggression | Excessive dopamine signaling may be clinically important. | Copper/zinc, methylation status, toxic burden, inflammation, sleep and metabolic monitoring. |
| Medication worked, then stopped | The drug mechanism may still be correct, but nutrient depletion, inflammation, hormonal change, toxic burden, sleep loss or elevated SAH may now be limiting response. | Repeat Walsh labs, SAM/SAH, vitamin D, copper/zinc, pyrroles/B6, CBC/CMP, thyroid and medication adherence/interactions. |
Common Medication and Nutrient Questions
What is the best antidepressant for undermethylation?
An SSRI may make the most mechanistic sense when high histamine, OCD, rumination and low-serotonin symptoms dominate. Bupropion may fit better when low dopamine, fatigue and motivation are the main problems—provided copper-related norepinephrine excess is absent.
Why did my antidepressant work and then stop?
The initial mechanism may still be appropriate, but low vitamin D, zinc/B6 depletion, copper overload, elevated SAH, inflammation, poor sleep, hormonal changes or drug interactions can reduce the response.
Why does Adderall help ADHD?
Amphetamine increases dopamine and norepinephrine in brain circuits responsible for attention, working memory and impulse control. It helps when baseline signaling is below the optimal range, but can worsen anxiety when norepinephrine is already excessive.
Can nutrient treatment reduce medication needs?
Sometimes. Correcting zinc, B6, vitamin D, copper imbalance, methylation inhibition, poor protein intake or toxic burden may improve the same systems the medication is supporting. Any dose reduction still requires the prescriber.
Stabilize First. Correct the Biochemistry. Reassess Medication Last.
The safest sequence is to maintain protection during periods of severe instability, identify the Walsh and nutrient pattern, begin targeted supplementation, and then reassess medication choice and dose after laboratory values and symptoms have improved. Only when stability is sustained should the patient and prescribing clinician consider tapering or discontinuation.
The goal is not necessarily “no medication.” The goal is the least medication necessary for safety and function, supported by the strongest biochemical foundation possible.
Frequently Asked Questions About Antidepressants, ADHD Medication and Nutrients
Can Walsh testing identify the best antidepressant?
It cannot select a drug directly. It may show whether the mechanism of an SSRI, dopamine-enhancing drug, norepinephrine-enhancing drug or dopamine-blocking drug is more or less consistent with the biochemical pattern.
Are SSRIs a poor choice for overmethylators?
In the Walsh model, many low-histamine overmethylators already show excessive or poorly regulated serotonin/dopamine activity and may worsen with additional serotonergic stimulation.
Can stimulants be problematic in copper overload?
Yes. Amphetamine and methylphenidate raise dopamine and norepinephrine. When copper overload already favors excessive norepinephrine, stimulants may worsen panic, insomnia, irritability or cardiovascular symptoms.
What should be tested when medication stops working?
Whole-blood histamine, SAM/SAH, methionine, homocysteine, copper, ceruloplasmin, zinc, pyrroles, vitamin D, CBC, CMP, thyroid, iron status, sleep and medication interactions may all be relevant.
What is the best antidepressant for depression?
There is no universally best antidepressant. The most appropriate choice depends on symptoms, past response, side effects, safety factors and whether the dominant biochemical pattern suggests low serotonin, low dopamine, excessive norepinephrine or excessive neurotransmitter activity.
What antidepressant should I take for an MTHFR mutation?
An MTHFR variant does not select an antidepressant. Functional testing with homocysteine, MCV, whole-blood histamine, SAM and SAH is more informative than using the SNP alone to assume a methylation diagnosis.
What is the best medication for anxiety?
The answer depends on the cause of anxiety. Low serotonin, copper-related high norepinephrine, stimulant activation, overmethylation, pyroluria and withdrawal can all produce anxiety but do not logically point to the same medication.
Why did my antidepressant stop working?
Possible reasons include changes in illness severity, adherence, metabolism, sleep, hormones, inflammation, vitamin D, zinc/B6 status, copper balance, elevated SAH, toxic burden or medication interactions. A new evaluation is more useful than assuming the dose simply needs to be increased.
Can nutrients make antidepressants or stimulants work better?
Correcting a documented nutrient or biochemical problem may improve neurotransmitter synthesis, receptor function, methylation, energy metabolism and medication tolerance. Nutrient treatment should be individualized rather than added blindly.
Should nutrients be started before antidepressants are stopped?
Usually, yes. In patients who are unstable or at risk, the safer sequence is to maintain necessary medication, test and correct biochemical abnormalities, allow time for stabilization, and only then consider a slow prescriber-guided taper.
What if the patient is suicidal, psychotic or potentially dangerous?
Immediate psychiatric safety and stabilization take priority. Nutrient and Walsh treatment may be added, but medication or higher-level psychiatric care should not be delayed or removed when it is needed to protect the patient or others.
Second Opinion Physician is a nutrient-based medical practice. This page does not prescribe a specific drug or advise abrupt discontinuation. Patients with suicide risk, psychosis, mania, severe instability or danger to self or others require immediate psychiatric assessment. Medication selection, continuation, dose changes and tapering require the prescribing clinician.