Lyme Disease, Biofilms, Ozone Therapy and Chronic Infection Burden
Lyme disease is usually discussed as a tick-borne infection caused by Borrelia burgdorferi, but many patients searching for Lyme answers are really asking a broader question: why do symptoms sometimes persist, why are biofilms discussed, and where do oxygen, ozone therapy, inflammation, detoxification, and chronic infection burden fit?
This page explains Lyme disease, Borrelia biofilms, standard antibiotic treatment, post-treatment symptoms, and newer supportive approaches that patients often research, including NAC, enzymes, EDTA, hyperbaric oxygen, ozone therapy, and rectal ozone insufflation as a practical at-home alternative to costly office-based IV ozone approaches. It also includes the Dr. Alan MacDonald video on Lyme biology and links to SOP ozone therapy resources, including Dr. Frank Shallenberger, Dr. Robert Rowen, and home ozone safety.
Ozone therapy for Lyme disease, Borrelia and biofilms
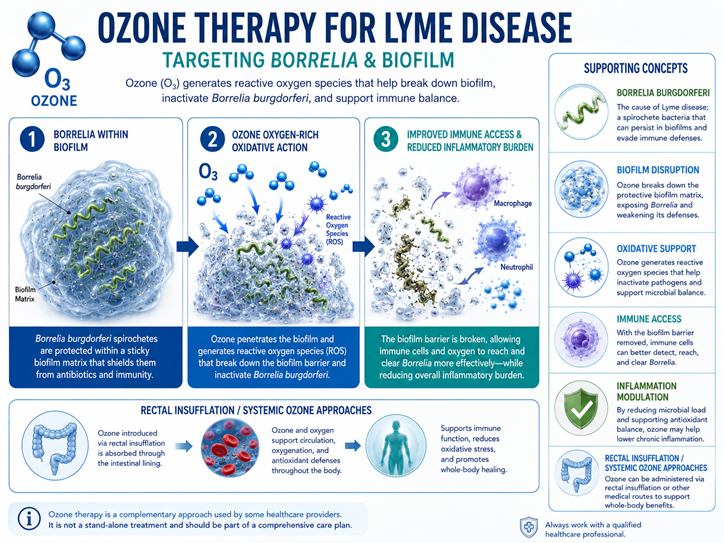
The infographic below summarizes the patient-education concept behind ozone therapy for Lyme-related chronic infection burden: ozone creates reactive oxygen species that may help disrupt biofilm structure, expose protected Borrelia organisms, support immune access, and reduce inflammatory burden. This is a mechanistic and supportive-care discussion, not a claim that ozone cures Lyme disease.
ozone.therapy.lyme.disease.png
What is Lyme disease?
Lyme disease is an infectious illness caused primarily by Borrelia burgdorferi and transmitted by infected black-legged ticks. Early Lyme disease may cause a bullseye-like erythema migrans rash, fever, chills, fatigue, headache, muscle aches, joint pain, and swollen lymph nodes. If the infection disseminates, it can involve the nervous system, joints, heart rhythm, and inflammatory symptoms.
Standard treatment usually involves antibiotics such as doxycycline, amoxicillin, or cefuroxime. Early treatment is important because untreated Lyme disease can become more complicated. Some patients continue to report fatigue, pain, cognitive symptoms, sleep disruption, and inflammatory symptoms after antibiotic treatment, often described as post-treatment Lyme disease syndrome.
Video: The Biology of Lyme Disease with Dr. Alan MacDonald
The video below is The Biology of Lyme Disease: An Expert’s Perspective. The speaker is Dr. Alan MacDonald, a retired physician and board-certified pathologist in anatomic pathology and clinical pathology. The interview discusses Lyme disease controversies, chronic Lyme disease, Borrelia forms, biofilms, microscopy, brain tissue findings, Alzheimer’s-related questions, and flaws in Lyme disease testing.
Who is the author or speaker?
The video features Dr. Alan MacDonald, MD. He is known in the Lyme community for pathology work involving Borrelia, biofilms, microscopy, tissue studies, and the possibility that certain chronic neurologic conditions may involve infection-related pathology. His views are not the standard CDC treatment position, but they are important for understanding why biofilms and persistent infection remain part of the Lyme discussion.
The role of biofilms in Lyme disease
Biofilms are protective microbial communities embedded in a matrix of extracellular material. In other chronic infections, biofilms are well known to help microbes tolerate antibiotics, resist immune attack, and persist in difficult environments. Borrelia burgdorferi has been shown in laboratory studies to form aggregates and biofilm-like structures, and later work has examined Borrelia biofilm markers in human tissue.
Biofilms may not explain every case of persistent symptoms after Lyme treatment. They are one possible mechanism among many, including immune dysregulation, inflammation, tissue injury, coinfections, persister cells, gut disruption, mitochondrial stress, and toxic burden. The practical point is that some Lyme patients may need a broader strategy than antibiotics alone.
Biofilm matrix
The biofilm matrix can shield microbes from immune attack and reduce exposure to antimicrobial agents.
Persister forms
Borrelia may shift forms under stress, and persister-like forms are part of ongoing research into treatment failure and post-treatment symptoms.
Immune activation
Even after antimicrobial treatment, inflammatory and immune patterns may continue to drive symptoms.
Biofilm treatment approaches patients often ask about
Biofilm strategies are usually supportive or adjunctive. They should not replace appropriate Lyme disease diagnosis or standard antibiotic care when antibiotics are indicated. They are best considered as part of a broader plan that includes infection assessment, inflammation, gut health, detoxification capacity, mitochondrial function, sleep, nutrition, and immune resilience.
NAC
N-acetylcysteine is often discussed because it supports glutathione and may influence mucus-like or extracellular matrix structures. It is also useful in oxidative stress strategies.
Enzymes
Serrapeptase, lumbrokinase, nattokinase, and other enzymes are often discussed for fibrin, mucus, and biofilm matrix support, especially in chronic inflammatory states.
EDTA and minerals
EDTA is discussed because minerals can stabilize some biofilm matrices. It must be used cautiously because it can also affect beneficial minerals.
Oxygen-based therapies
Hyperbaric oxygen and ozone therapy are discussed because oxygen tension, oxidative signaling, and microbial redox stress may influence biofilms and immune response.
Ozone therapy for infections, biofilms, Lyme disease and chronic inflammation
Ozone therapy is controversial, and it should not be presented as a stand-alone Lyme disease cure. A careful functional medicine discussion frames ozone as a redox-support tool. Ozone’s oxidative properties may be relevant to microbes and biofilms, while lower-dose systemic ozone approaches are usually discussed in relation to immune signaling, mitochondrial function, oxygen utilization, glutathione response, inflammation modulation, and detoxification tolerance.
For SOP patients, ozone therapy is most relevant when chronic infection burden overlaps with gut dysbiosis, biofilm concerns, inflammatory symptoms, chemical sensitivity, mold or toxic burden, poor recovery, fatigue, pain, brain fog, and mitochondrial weakness. Office-based methods such as major autohemotherapy, 10-pass ozone, and EBOO can be expensive and difficult to repeat. Rectal ozone insufflation deserves special attention because it may offer a more affordable, convenient, repeatable home route when properly instructed.
Rectal ozone and gut pathogens
Rectal ozone is commonly discussed as a non-IV route for gut-focused and systemic support. It still requires route-specific instruction and proper ozone-compatible equipment.
Biofilm burden
Ozone has antimicrobial and antibiofilm properties in experimental settings, but clinical Lyme use remains investigational and should be integrated carefully.
Chronic inflammatory load
Ozone is often discussed as a controlled oxidative signal that may stimulate adaptive antioxidant and inflammatory-regulating pathways.
Rectal ozone insufflation: the practical alternative to expensive IV ozone
One of the biggest obstacles with ozone therapy for Lyme disease, biofilms, chronic infection burden, and chronic inflammation is not only medical controversy. It is cost and access. Major autohemotherapy, 10-pass ozone, EBOO, IV ozone, and other clinician-administered ozone methods can be expensive, time-consuming, and difficult to repeat often enough to create a steady redox-conditioning effect.
Rectal ozone insufflation is important because it changes the practical equation and is shown conceptually in the infographic above. It is non-IV, can be performed at home when personally instructed, uses far less equipment than blood-based ozone methods, and may allow frequent or daily ozone exposure without the financial burden of repeated office-based IV ozone sessions. This is why both Dr. Frank Shallenberger and Dr. Robert Rowen are often referenced by patients researching rectal ozone as an accessible alternative to more expensive ozone procedures.
More affordable than 10-pass or EBOO
10-pass ozone and EBOO require physician visits, IV access, special equipment, and repeated sessions. Rectal insufflation is usually much more practical for ongoing home use.
Daily redox support is the advantage
The central practical advantage is frequency. A patient may be able to use rectal ozone regularly at home, while IV ozone may be limited by cost, travel, time, and vein access.
Relevant to gut pathogens and inflammation
Rectal ozone is especially relevant when Lyme-like symptoms overlap with gut dysbiosis, biofilm concerns, systemic inflammation, detoxification stress, and poor recovery.
Important distinction
Rectal ozone should not be presented as clinically proven to outperform IV ozone, 10-pass ozone, or EBOO for Lyme disease. The stronger claim is practical: rectal ozone may be the most accessible, affordable, repeatable route for patients who have been instructed in home ozone therapy and need regular redox support.
Diagnosis of Lyme disease and testing limitations
Standard Lyme testing typically begins with antibody testing, often followed by confirmatory testing when indicated. PCR testing may be used in selected tissue or fluid contexts, but it is not a general screening test for all chronic symptoms. The major clinical challenge is that symptoms can persist for multiple reasons, and not every chronic symptom pattern is proof of active Borrelia infection.
ELISA / EIA
Often used as the initial screening test for antibodies against Borrelia burgdorferi.
Western blot / immunoblot
Used as confirmatory testing in many Lyme disease testing algorithms.
PCR and specialty testing
May be useful in selected contexts but does not replace clinical judgment and standard diagnostic criteria.
How SOP frames Lyme, biofilms, ozone and toxic burden
SOP patients often present with overlapping patterns: chronic infection history, mold exposure, gut dysbiosis, chemical sensitivity, insomnia, brain fog, fatigue, pain, low stress tolerance, inflammatory symptoms, and poor recovery. In those cases, the question is not only “what kills Borrelia?” The broader question is how to reduce the total inflammatory, microbial, oxidative, and toxic burden while supporting detoxification, mitochondria, minerals, methylation, sleep, gut health, and immune resilience.
Important safety and regulatory cautions
Ozone therapy is controversial and is not recognized by the FDA as a proven treatment for Lyme disease or chronic infection. Ozone gas can irritate or injure the lungs and should never be inhaled. IV ozone, blood ozone, injections, dental ozone, and Prolozone-style treatments require trained clinicians and should not be attempted at home.
- Do not inhale ozone gas.
- Do not use ozone as a replacement for appropriate Lyme disease evaluation or antibiotic care.
- Do not attempt IV ozone, blood ozone, or injections at home.
- Use only ozone-compatible supplies and route-specific guidance.
- Complex Lyme disease, neurologic symptoms, heart symptoms, pregnancy, severe infection, or major medical instability require physician care.
References and related resources
Frequently asked questions
Who is in the Lyme disease video?
The video features Dr. Alan MacDonald, MD, a retired physician and board-certified pathologist in anatomic pathology and clinical pathology. He discusses Lyme disease biology, Borrelia forms, biofilms, microscopy, brain tissue findings, and testing limitations.
Can Borrelia form biofilms?
Research shows that Borrelia burgdorferi can form aggregates and biofilm-like structures in laboratory settings, and additional studies have examined Borrelia biofilm markers in human tissue. The clinical significance remains debated.
Does ozone therapy treat Lyme disease?
Ozone therapy should not be described as a Lyme disease cure. It is better discussed as a redox-support tool that may be relevant to microbial burden, biofilms, inflammation, mitochondria, glutathione response, and detoxification tolerance.
What is the connection between ozone and biofilms?
Ozone has antimicrobial and antibiofilm properties in experimental settings. Clinical use for Lyme disease remains investigational and should be supervised by a qualified clinician.
Why discuss rectal ozone instead of only IV ozone, 10-pass ozone, or EBOO?
Cost and frequency are major obstacles with IV ozone, 10-pass ozone, and EBOO. Rectal ozone insufflation is non-IV, more affordable, easier to repeat, and may allow regular home ozone exposure when personally instructed. It should be viewed as a practical access advantage, not as proof that it outperforms IV ozone for Lyme disease.
Is daily rectal ozone better than occasional IV ozone?
Daily or frequent rectal ozone may offer a practical advantage because repeated redox signaling can be done at home without repeated IV visits. However, there are no large clinical trials proving that daily rectal ozone is superior to 10-pass ozone, EBOO, or major autohemotherapy for Lyme disease.
Should biofilm therapy replace antibiotics?
No. Antibiotics remain the standard treatment for Lyme disease when indicated. Biofilm strategies may be considered adjunctive and should be integrated with proper diagnosis, medical care, and safety monitoring.
This page is educational and does not diagnose, treat, cure, or prevent Lyme disease or any infection. It is not a substitute for individualized medical care. Severe neurologic symptoms, heart symptoms, fever, acute infection, pregnancy, or worsening illness require prompt medical evaluation.