Understanding Folic Acid, Methylation, and Related Mood Disorder Symptoms: Insights from Dr. William Walsh.
Contrary to popular belief, methylation status is not solely determined by MTHFR positive genetic mutations, and high homocysteine does not necessarily mean someone is low in folates. Folates, including methylated and non-methylated forms, can improve methylation, but they may lower serotonin activity by increasing serotonin reuptake transport proteins.
Individuals who are undermethylated do not usually have low folic acid levels, and if they genuinely experience undermethylation, they are likely to suffer from mood disorders due to low serotonin activity. A whole blood histamine and homocysteine test can help determine one's true methylation status, and a Walsh Approach can help increase serotonin activity in undermethylators while avoiding folates.
Individuals with MTHFR genetic SNPs' may take methylated B vitamins to improve homocysteine and prevent neural tube defects. But with depression and mood disorders, methylated folates can be problematic.
Dr. William Walsh, the founder of the Walsh Research Institute in Chicago, has conducted educational workshops on epigenetics, depression, and methylation. His research sheds light on the complex relationship between folic acid, methylation, and mood disorders.
2 Minute video. When it comes to treatment for mental disorders, an individual’s overall methylation status is most important. Dr. Walsh explains why genetic testing cannot determine which SNPs are dominant. He recommends testing for the net effect of the various SNPs, which include SAMe/SAH ratio or whole blood histamine.
Advanced Nutrient Therapies for Brain Disorders- William Walsh (Nov 2015)
1.5 hour video recorded at Silicon Valley Health Institute. This presentation discusses the power of nutrients to normalize neurotransmitter synthesis, regulate gene expression of enzymes, and combat oxidative overload.

Symptoms associated with undermethylation and overmethylation:
Undermethylators
Low Serotonin Activity
"Normal Folate Depression"
- Chronic depression
- Autism
- Oppositional Defiance
- Obsessive Compulsive Disorders
- Psychosis prior to the onset of depression or other conditions.
- Strong willed
- Seasonal allergies
- High libido
- Competitive in sports
- Overachiever prior to the onset
- Protein deficiency and vegetarian diets
- Tends to do better on SSRI medications
- Responds well to antihistamines
Overmethylators
Elevated Serotonin Activity
"Low Folate Depression"
- Acute depression
- Panic disorders
- ADHD
- High anxiety
- Paranoia
- Schizophrenia with auditory hallucinations
- Dry eyes
- Highly artistic, sociable and empathetic
- Poor response to SSRI medications
- Poor response to antihistamines
- Food and chemical sensitivities
- Not typically competitive
- Builds muscle mass easily
Educational Posts on Methylation
Useful Methylation and Histamine Testing Labs
Walsh Approach Single Tests
Walsh Approach Test Panels
Methylation Test Panel – Whole Blood Histamine & Homocysteine

Walsh Approach Test Panels
I have the MTHFR C677T gene mutation.
I have been taking B12, methylfolate & 800 mg per day of SAMe. It worked to get some health issues cleared up.
I have done well with this treatment for several years but have recently developed constant diarrhea which I have had for 3 mos. Nothing seems to help. I’m currently on medical leave from teaching. I also have always had high levels of inflammation in my gut, allergies & food sensitivities. Help! I have lost over 15 lbs and did not have much weight anyway, being a competitive distance runner athlete. I’m not doing much exercise lately which may contribute to issue. Have taking care of aging parents. They are doing better than me! Some family members have had bouts w depression. I’m doing ok in that aspect.
Any suggestions that might help me to clear up diarrhea?
Hi Linda, SAMe and folate have opposing effects on serotonin and dopamine activity. Suggest testing histamine levels to determine status of methylation before taking either of these supplements.
What test do you run to check histamine levels
And
What about whole blood histamine to determine methylation status?
My gf is bipolar and we started the Walsh nutrient therapy 3 months ago. She is undermethlated with a slight copper overload. We did the blood test to determine these results with a nuturalpath who does the Walsh protocol. She has had three psychosis breaks since Jan 2018 and each resulted in hospitalization. She is taking 80mg of latuda at supper, 1200mg of lithium and 15mg of olanzapean at night. The nutrient protocol recommendations are 10,000IU vitamin A, P5P, Vitamin E, liposimol Glutithione, Sam-e, Zinc. Her has
Complained about stomach upset for months
And still has some psychotic thoughts such a spirits and demons needing to be fought. Can I do more the help with her stomach and brain functions now that we know she is under methylated? I’m thinking shamanic healer for emotional trauma in conjunction with psychologist and olive leaf with a probiotic? She wants to lose weight and has had a very difficult time doing that.
This article currently states that 18 percent of depressed patients are overmethylators with low serotonin and dopamine. I believe this should say elevated levels of serotonin and dopamine with low levels of histamine.
I had a minor surgery 3 years ago and woke up in a state of panic and felt like nothing was real for about 7 days. When the acute episode ended I started becoming depressed, suffered from chronic anxiety and panic attacks daily, i took a pediatric dose of xanax just so I didn’t feel like I was dying 24/7. I eat very well, am a whole foods nutritionist but nothing worked naturally. I thought I was loosing my mind. I finally started zoloft and after 2-3 months it started to work. For 2.5 years I was fine and I was titrating off the whole time because I felt normal again, I had a history of anxiety but kept it in check for 20 years with diet and exercise, absolutely no medication. So I thought that 3 months was just an episode, I had recently moved 1000 miles away from any family with 3 children, just had my 3rd when it happened and I was lowered to 25 mg then 15 mg of zoloft over the course of a year . When I finally stopped the zoloft all of the symptoms reappeared. I tried everything, exercise, a host of natural supplements, b vitamins, rhodiola, ashwaganda, mag taurate but nothing worked and I was again in the same state. I am now on 50 mg of zoloft and feeling better but I went to a functional medical doctor and had extensive testing done. No smoking gun, my protein was low, some viral concerns and inflammation and my kidneys were not doing that well but everything else was fine, my B vitamins, vit D, my hormones. I want off this medication because I know it is not correcting the real issue but I am so afraid to go through that again. This doctor says he is going to work on methylation and my neurotransmitters. It is going to cost 4-5 thousand dollars and I just feel so defeated.
The history is relevant in order to determine symptoms, medication history and past results. However, to get a good idea of the biochemistry associated with neurotransmitter levels a Walsh-trained physician and a Biotype blood panel should provide actionable information.
Thank you for spotting that typo.
What you describe is not a full protocol for undermethylators. Further complicating the issue are these medications. I suggest you coordinate with the Walsh Practitioner and your prescribing physician to determine if medicine levels can or should be adjusted. Before changing doseages of medications or supplements it would be helpful to see how the labs and symptoms have changed, if at all, since she has started supplementation.
Whole blood histamine is ordered to determine methylation status. Typically this is ordered with homocysteine in order to determine best supplement plan.
I am definitely high in histamine, and low in neurotransmitters. I am an undermethylator. My test results came back high in methyl-histamine; I have all the symptoms of an undermethylator (ie…previous diagnosis of Interstial cystitis that went away after time, flusing, itching skin when I run, anxiety, racing thoughts, etc…… However, when I try to supplement such as SAMe or 5HTP, I get very nauseous and wired. I am already wired from being undermethylated and can’t take more anxiety from SAMe and Nausea from 5 HTP. What other supplements should one take if the suggested supplements for an undermethylator make him/her wired and nauseous? Is this common?
It is important when treating elevated histamine to know copper/free copper status, vitamin D levels and to know one’s homocysteine levels and cardiac risk factors. Treating with SAMe or methionine is not a complete methylation program and may cause problems if other issues are not addressed first. Best to start a treatment plan with these possible issues addressed. Once corrected, if imbalanced, it is easier to handle SAMe and methionine. Nausea is common with digestive inflammation, yeast and leaky gut. 5HTP is not part of our protocol even with undermethylators.
17 year old son, recently diagnosed with depression, OCD. He hid it for several months, until suicidal ideation became a factor & he informed us. We immediately sought treatment via psychological & psychiatric avenues. Evaluation recommendations include weekly counseling sessions & medication (currently 2mg/day Abilify for past 2weeks). I’ve insisted on getting to the root cause, which is a slow, painful process. So far only managed to get MTHFR test (no abnormality there) & neurotransmitter panel, which showed elevated histamine, yet normal to slightly high serotonin, dopamine & norepinephrine. However, epinephrine & PEA were low. Began supplementation, before getting testing, with magnesium (insomnia), D3, C, multivitamin, B complex, inositol, & fish oil. Within last 2weeks, per Dr. recommendation, added adrenal support, benedryl, phenelyalanine & Abilify. His mood has seemingly improved in the last week 1/2. I still want to get to the root issue, as I believe depression is a symptom & not a diagnosis, & wonder what further testing is recommended, as I have to push to get it done. Also regarding methylation status, he has conflicting symptoms. So, I’m trying to determine cause of histamine elevation(allergy, stress, dehydration, etc…) & should I be more concerned with why it’s not being broken down. Also, benedryl? He exhibits no allergy symptoms. Sorry, this is so long, I’m trying so hard to advocate for my son & get him well & happy again. Any advice would be greatly appreciated. Thank you.
Hello . I m from india . First i dignosed with ocd , sexual obsessions . Got 150mg sertaline and aripiprazole 5 mg . Took 4 years . I thought i m ok with these medicines but it was hypomania . I realized and stopped medicines . Then i got bipolar 2 dignosis . No lithium lamictal worked for me . Just made me more depressed . I tried vitamin minerals then but nothing working . My folate level is 0.8 and b12is 238. What should i do . Plz tell.
Hi! Could you explain why neurotransmitter precursors such as tryptophan/5-HTP or Tyrosine/Phenylalanine are not mentioned in your protocols? Undermethylators are said to be low on neurotransmitters and it would seem like they could only help in their production. Is it OK to take them?
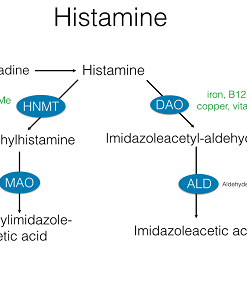
As Walsh describes in his physician trainings, the issue is not with insufficient levels of neurotransmitters; the issue is with reduced activity. With undermethylation the problem is due to an excessive expression of SERT and DERT neurotransmitter reuptake promoters. Excessive reuptake is why SSRI drugs, reuptake inhibiters have become the main focus of antidepressant medicine research and therapy. When we thought diminished levels of neurotransmitters were the issue, the treatment was MAO inhibitors; this is no longer the desired approach.
There are a number of conflicting strategies here. While histamine is a co-factor in depression, it is not likely the cause. MTHFR does not tell us much about methylation status, nor should it be a recipe for supplementation. Suggest the methylation panel of histamine/homocysteine – this will tell us if your histamine is elevated due to undermethylation. Supplements that improve methylation, sans folates, will be best if your whole blood histamine is elevated.
My daughter got her period less than a month ago and immediately started experience intruding/racing thoughts and severe anxiety. This has been going on for three weeks with very little relief. What is your recommended course of action at this point. Do you have any recommendations for someone to run comprehensive blood work to see what supplements and nutrients will give her some relief? We are in San Antonio TX. Thank you!
Hi Ana, I’m sorry to hear about your daughters condition. Hormone changes frequently lead to mood disorders due to the Biotype Dr Walsh refers to as “copper overload.” Combined with low vitamin D and or elevated whole blood histamine, this is a very common cause for intruding thougths and severe anxiety. Depending on urgency you may want to see a local physician and have her evaluated to be sure she is not in any danger. If not so urgent, I would consider test Copper Overload Biotype, Histamine and Vitamin D levels. In case you would like my assistance with lab selection and assessment of results, I am following up with an email to introduce you to the protocol.
Yes, that’s a great questions. We don’t useS serotonin precursors in the Walsh approach for a similar reason that pharmaceutical MAO inhibitors are used less often these days than SSRI drugs. The production levels are less important than the activity or reuptake activity of the neurotransmitters. Methylation is important with regards to serotonin activity from the epigenetic influence it has on the DNA that transcribes serotonin reuptake transport proteins. Undermethylators produce a high amount of these reuptake proteins, which lowers the effectiveness of the neurotransmitters. Most undermethylators respond better to methylation for its epigenetic influence on increasing methionine or methyl groups that act on the DNA.
Folates are not recommended for persons who are depressed or with similar symptoms unless a whole blood histamine test or methylation panel has definitively shown that one is OVERmethylated. We do not use folates in undermethylated persons because it acts on the reuptake protein production, lowering production and thereby increasing reuptake, which is good for overmethylators, who have high levels of serotonin and low folates.
Hello,
i would please like to ask a question about what happens in the case that someone, due to homozygous C677T MTHFR, has very Low Folate in blood tests, and also has high homocysteine in blood tests. The normal response would be to take more folate to correct the folate deficiency and also to lower the high homocysteine. But, what happens if this person is also an undermethylator? This would be something of a paradox, because this person should take more folate to correct the folate deficiency and lower the high homocysteine, but the extra folate would cause him/her to have what dr. walsh says a serotonin reuptake promotion so there would be a worsening of this person’s existing psychological symptoms (depression/anxiety or ocd). What should happen in such a case as regards to supplements? And also shouldn’t such a person avoid SAMe, because it would make the homocysteine rise even more?
Thank You
These are all good questions. Folate tests serum or blood are not reliable or else expensive. Values fluctuate and testing is not consistent. Homocysteine, homozygous SNPs and RBC morphology are helpful to determine but Walsh’s research indicates that most who are genuinely undermethylated (elevated WB Histamine) are not folate deficient. Most often it is the overmethylator who is and they frequently have the macrocytosis to confirm. I suggest determining methylation status with a whole blood histamine level and make a folate assumption based on that plus CBC and homocysteine. Chronic folate deficiency is reflected by an almost certain macrocytosis, as long as B12 deficiency is ruled out. Folate should be taken when levels are low and plus macrocytosis with normal B12, plus elevated homocysteine and/or when planning conception. FYI, homocysteine may be lowered with TMG, serine, B6 and NAC – it’s not just about B12 and folate or the genetic SNPs. If an undermethylator is with MTHFR / C6771, plus macrocytosis and low folate, then a low dose of folic acid, if it doesn’t significantly worsen a bad case of depression, may be tolerated and necessary. There are a lot of ifs and what ifs because there are many functions that biochemistry performs in the body and people have unique variables. Get a WB Histamine, CBC and homocysteine, plus a Walsh trained doc to review your history. And start slowly. Nutrients are much more forgiving than pharmaceuticals.
Hi,
I have been very depressed and anxious for as long as I can remember. I started a new supplement today, folinic acid. I can hardly put into words how great I feel, I hope this continues to work for me. I feel like a totally different person, the horrible black cloud has lifted. I am hoping that this bit of info can be helpful to others who are suffering as I have. God bless and don’t ever give up.
Please be careful supplementing with folates. Most people do well when depressed for the first few days but a signifiant number then notice a worsening of mood related symptoms. The reason is that it will quickly increase methylation but then it acts on the reuptake of serotonin to decrease the activity of serotonin. This is more pronounced than the increase in production of serotonin from improved methylation. Suggest testing whole blood histamine to know what is your actual methylation status prior to taking folates, niacin, choline and dmae.
Sorry for the delayed reply. I was not aware of this message. Severe anxiety with menstrual changes may be due to estrogen and copper imbalance. The Comprehensive Biotype panel will help determine copper overload status as well as methylation and other factors such as Vitamin D levels. This is the best place to start.
This is Sandy again, from 1-10-20 post. You were absolutely correct, the wonderful feeling only lasted three days. Yesterday I woke up feeling like a truck had run over me, depressed, and had a horrific headache that lasted all day. Having those wonderful three days has given me a glimpse of how my future could look, the happy-go-lucky gal is fighting to get out. I have made an appointment for consultation with you and am excited about talking to someone who understands this yucky condition.
Hi Sandy, Thanks for your feedback. You have experienced the difficulty of taking folic acid for a mood disturbance without first ascertaining methylation status. Your response demonstrates why so many others do poorly by taking multi vitamins and b-complex when depressed, prior to utilizing histamine as a measure of true methylation status. Typically folates, niacin and DMAE are restricted to overmethylators (low WB histamine), those with high homocysteine (non responsive to B6, and B12), macrocytosis (non responsive to B12), and low serum folate levels with homozygous methyl enzyme genetic SNPs.
I’ve struggled with leaky gut lately, and have been on a strict anti-inflammatory diet with low carbs since november, along with olive leaf and other antifungals. I have been taking multivit, C-vit, E-vit, and then added B-complex in january. Since january my histamine intolerance (which I didn’t have before november) has gone sky-high, and I have become very sensitive. Since january I have also been struggling with stress, anxiety and depression. My folate level was slightly elevated before I started B-complex.
I have now stopped B-complex and multivit due to folate. I believe this indicates I am under-methylating?
I was considering starting SAM-e. But should I do ant tests first?
I’m an undermethylator, depressed and homozygous C677T. My homocysteine levels aren’t fine. 5-MYHF, folinic acid, Folate, B’s and multiplied vitamins often make me feel worse. What would you recommend I take?
Yes, the test is important. Plasma histamine and symptoms related to histamine intolerance do not always imply someone has high Whole Blood Histamine. Treating incorrectly can have the opposite of a desired effect. That can be particularly deleterious with depression, schizophrenia, psychosis and other mood disorders.
Take the Whole Blood Histamine test. Best to know for sure if you are an undermethylator. Genetic testing does not provide that information. It may show a defect in one or two of many genes that influence methylation but a better test is the WB Histamine or the Doctors Data Methylation Panel.
I would like to know if my daughter is undermethylated or overmethylated. She had a breakdown in 2013 and had to be hospitalized. She lost over 15 pounds on a small body frame, which I think helped with the physchosis. In the hospital they put her on halpidol, seroquil, depakote and different medications for physchosis and bipoplar disorder. Since, she has continued on and off using seroquil and depakote, but keeps experiencing depressive moods, with negative thougts and beliefs. Can you help with what supplements and vitamins, food natural remedies will help to get off this horrible medication.
Yes. The goal with biochemical evaluation and use of supplements is to help patients recover from mood disorders and get off of all medications. The first step is to do the Comprehensive Biotype Lab Panel and complete a questionnaire for evaluation. Then the process of supplementation begins. After some weeks, when mood has stabilized we then consider working with prescribing physician or primary doctor to ween off medicines.